
The success of clinical pharmacy in team-based care depends on effective partnerships and collaborations. Clinical pharmacists collaborate with our care team colleagues, with patients and their caregivers, and with other members of the pharmacy profession—whether within an institution or the community. Our ability to work together is a key component of achieving optimal patient outcomes.
Effective interprofessional teams are typically focused on a defined goal—achieving the best outcome for that patient and doing so efficiently and safely. However, if individual members of the team lose sight of that big-picture goal and become too focused on day-to-day challenges, or individual practitioner/discipline-specific needs, achievement of the overarching goal can be negatively affected. Collaboration among professional organizations must similarly be designed around a focused goal to be most productive.
During the past 5 years, ACCP has developed some important organizational partnerships and collaborations to help achieve our overarching goal of providing comprehensive medication management (CMM) by qualified and appropriately credentialed clinical pharmacists. Patrick Lencioni, in his book Silos, Politics and Turf Wars: A Leadership Fable About Destroying the Barriers That Turn Colleagues into Competitors, describes in detail how to identify and remove barriers that prevent achievement of an important goal (San Francisco: Jossey-Bass, 2006). He provides an important caveat that is pertinent to how ACCP views its current partnerships and collaborations. In Lencioni’s view, the most essential component of an effective collaboration is a compelling goal that provides context for all team members to work in a single direction rather than pursuing siloed, individual goals. And of course, CMM can only be optimally accomplished through meaningful interprofessional, non-siloed collaboration.
This prompted me to think more deeply and ask, “But is ACCP really a collaborative organization?” After all, the College has often been questioned—and criticized—for its lack of formal participation in the Patient Access to Pharmacists’ Care Coalition (PAPCC) since that coalition was established in 2013. However, it is important to recall that the option for the College to participate in the PAPCC was made conditional, with the stipulation that ACCP abandon its CMM Medicare reform initiative and supporting policy framework that was developed in collaboration with other health care stakeholders after several years of interprofessional foundational work. This focus remains a guiding principle for ACCP—so much so that we have allocated up to $2.5 million to fund research that will study the impact on patient outcomes of CMM provided by qualified clinical pharmacists in primary care medical practices. Although the PAPCC’s goal of recognizing all pharmacists as providers should be beneficial to patients if achieved, devoting ACCP staff time and resources to both that effort and the College’s primary priority (advancing CMM) would likely be unsuccessful, if the perspective of Lencioni is accurate. In short, we chose instead to channel our relatively limited human and fiscal resources toward support of what ACCP’s members do—namely, comprehensively manage patients’ therapy in collaboration with other members of the health care team.
Despite ACCP’s absence from the PAPCC, many other productive collaborations continue with colleague pharmacy organizations, medical societies, foundations, and other groups. The JCPP (Joint Commission of Pharmacy Practitioners) Pharmacists’ Patient Care Process document is an example of how diverse pharmacy organizations can meet a fundamental need of the profession (see https://www.accp.com/docs/positions/misc/JCPP_Pharmacists_Patient_Care_Process.pdf). Pharmacists will now be educated, trained, and expected to perform this patient care process whether in a hospital, community, nursing home, or other pharmacy practice setting. This standardized expectation for pharmacist practice is extremely important because it will establish what other health professionals and patients can expect from a pharmacist. It is an important foundational component toward ensuring that pharmacists have the expertise and skills to provide CMM. This document reflects the potential impact of a collaborative like JCPP, a group that includes major national pharmacist organizations, including ACCP. Through JCPP, these organizations meet face-to-face quarterly to discuss topics of relevance to the profession including health informatics, pharmacist workforce issues, interprofessional education and practice, and health care reform policies, to name but a few. This group will continue to work together to promote and implement the PPOC. The JCPP agenda for this year also includes the use of quality measures to determine patients’ medication-related outcomes. Through the Pharmacy Health Information Technology (HIT) Collaborative, an outgrowth of JCPP, national pharmacy organizations are also working together to ensure that pharmacists have needed access to patients’ health information. Although not always a perfect process, even competitor groups can achieve mutual goals when the outcomes of working together are compelling.
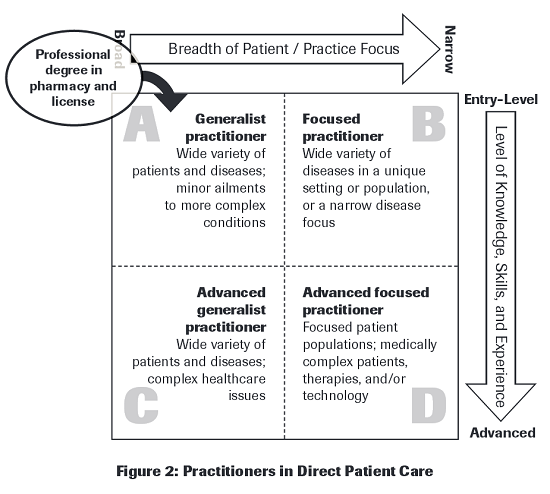
ACCP also serves an important role on the Council on Credentialing in Pharmacy (CCP). This group consists of organizations that have a commitment to quality in the areas of pharmacy accreditation, certification, and credentialing/privileging. In that forum, we have discussed the training and associated credentialing that serve as an important foundation for developing pharmacy practice competency standards. The work of this group led to the 2009 foundational document, “Scope of Contemporary Pharmacy Practice: Roles, Responsibilities, and Functions of Pharmacists and Pharmacy Technicians” (see http://www.pharmacycredentialing.org/Contemporary_Pharmacy_Practice.pdf). A noteworthy diagram in this document, reproduced here (“Figure 2”), illustrates the continuum from generalist practice to advanced specialty practice and the progressive levels of knowledge and experience required to assume certain practice responsibilities. This framework provides essential context for the training and experience needed to provide CMM. ACCP has been an important contributor to work products like this paper and others produced by CCP. Recent CCP meetings have considered how privileging processes can provide important structure and documentation to ensure that providers of direct patient care meet minimum practice criteria, as well as how competency statements for practitioners are being developed and used in other countries.
Of course, the organization leading specialist certification and specialty recognition is the Board of Pharmacy Specialties (BPS). Many ACCP members have served on BPS specialty councils, and their leadership and input have helped shape BPS’s approach to specialty recognition and specialist certification. Board certification remains one of the foundational components of our effort to advance CMM.
The National Academy of Medicine, formerly the Institute of Medicine (IOM), is another important collaborator for ACCP. For several years, ACCP staff have participated in the IOM Roundtable on Value and Science-Driven Health Care’s Best Practices Innovation Collaborative. The roundtable has produced papers important to practice innovation, most recently “Patients and Health Care Teams Forging Effective Partnerships” (see https://www.accp.com/docs/positions/misc/PatientsForgingEffectivePartnerships%20-%20IOM%20discussion%20paper%202014.pdf). This paper discusses how health professionals can more effectively include their most important partners—our patients—in interprofessional care. The key tenets of this paper illustrate the need for clarity in the role of the patient as a member of the health care team and the need to support shared and personalized decision-making that enhances communication among team partners while suggesting improvements to strengthen these efforts. Patients who were involved in developing this document indicated that health professionals still have much to learn in order to fully meet patients’ expectations for team-based care. We can be more effective in the provision of CMM if we understand how to truly meet patient needs.
In the quality arena, the College is a member of the Pharmacy Quality Alliance (PQA). ACCP members Mary Roth McClurg, Carla Cobb, and Joseph Vande Griend represented ACCP in 2014 work groups of PQA related to team-based care, behavioral health, and quality assessment measures. The work of PQA appears to be transitioning from a narrow focus on Part D/community pharmacy quality metrics to a broader medication use focus. Our ability to lead the development of metrics around CMM is a significant additional component of our overall goal.
Our partnerships with organizations outside pharmacy are similarly important to advancing CMM. ACCP staff have met regularly with senior staff of the American Academy of Family Physicians (AAFP) and have been included in interprofessional policy forums focused on a permanent solution to the Sustainable Growth Rate and Medicare physician payment reform issues. ACCP has also been involved in discussions on collaborating with AAFP on team-based CMM as part of the current CMS Transforming Clinical Practices Initiative.
Similarly, successful collaboration with the American College of Physicians (ACP) led to specific mention of clinical pharmacists as primary members of the clinical care team in a recent ACP policy paper (Doherty RB, Crowley RA; for the Health and Public Policy Committee of the American College of Physicians. Principles Supporting Dynamic Clinical Care Teams: An American College of Physicians Position Paper. Ann Intern Med 2013;159:620-6). A more recent collaborative relationship has been established with the American Congress of Obstetricians and Gynecologists (ACOG). ACCP is participating in their invited interprofessional task force on Collaborative Practice. Represented by ACCP member Marcia Buck and staff member Ed Webb, the task force is currently completing work on a policy document and practice toolkit, working alongside representatives of a range of health care provider organizations. See also the nearby story in this issue of the ACCP Report about our newest interprofessional collaboration—working with the Heart Failure Society of America and eight other medical and nursing societies to identify and establish benchmarks to improve the standards of quality care for individuals affected by heart failure.
Successful partnership with the Society of Critical Care Medicine (SCCM) has resulted in our organizations being recognized by BPS as joint providers of recertification activities for pharmacists who become Board Certified Critical Care Pharmacists. ACCP-SCCM educational initiatives at SCCM meetings will be delivered by interprofessional teams to further reinforce the importance of the role of clinical pharmacists as essential team members. Such support from specialist providers in medicine is fundamental to successfully achieving recognition of clinical pharmacist specialists and their provision of CMM.
Having posed the question above, I must conclude that ACCP is indeed a truly collaborative organization. Therefore, after reading this column, I hope ACCP members will appreciate the importance that the College’s leadership places on effective partnerships and collaborations—and how these efforts are yielding meaningful results and outcomes aligned with our core values and strategic goals.