Overview of the PRN
The Infectious Diseases Practice and Research Network (ID PRN) is composed of students, residents, fellows, pharmacists, and other clinical and research specialists who practice in the exciting area of infectious diseases. Serving 1162 total members, which include 132 students, 57 residents, and 18 fellows, the ID PRN is one of the largest PRNs within ACCP. Members are actively engaged in advancing pharmacy practice throughout an incredible variety of practice settings and believe strongly in education, research, credentialing, and professional stewardship. In addition, members are active and dedicated leaders on committees and executive boards within ACCP and other organizations.
Members of the ID PRN are dynamic, collaborative, supportive, and innovative. With a diverse and passionate membership base, the ID PRN recognizes how essential it is to engage members and consistently work together to extend the frontiers of clinical pharmacy practice. Our mission in our work is to disseminate knowledge and promote career opportunities for infectious diseases specialists to optimize patient outcomes and demonstrate the value of pharmacists across the health care continuum.
We encourage you to follow our social media pages to stay up-to-date with the latest practice advances in antimicrobial, antifungal, and antiviral pharmacotherapy! We can be found at:
- X/Twitter: @accpinfdprn
- Bluesky: @accpinfdprn.bsky.social
Opportunities and Resources
Resident and Fellow Opportunities
- Opportunity to serve on the Executive Committee
- To promote research and professional development, the ID PRN sponsors two $1000 awards to residents or fellows to present research posters at the ACCP Annual Meeting. Award recipients must present their original research in person at the ACCP Annual Meeting.
- Participate in the resident and fellow learner-led journal club series, which is presented on a monthly basis to national ACCP members, allowing trainees to develop presentation skills as well as gain invaluable feedback and insights into these topics
- Participate in the annual ID PRN mentorship program to serve as a mentor to a student
Student Opportunities
- Participate in the annual ID PRN mentorship program to be matched with a pharmacist, resident, or fellow mentor to help guide them in their professional development
All Trainee Opportunities
- Opportunities to serve on any ID PRN committee, including the Awards, Publications, Programming, Nominations, Networking, Research, and Social Media committees
The email list associated with ID PRN membership is active daily, inciting compelling clinical discussions and bringing attention to critical issues in practice. Networking is promoted through email list involvement, social media outlets, Annual Meeting attendance, pharmacy conference social events, research collaborations, and more. We welcome all who are interested in infectious diseases, even if it is not their current or primary practice area. The ID PRN website has great tools and resources for resident and student members. It also contains the contact information for all Executive Committee members. Please do not hesitate to reach out to us at [email protected]!
When the Label Does Not Fit: De-labeling Penicillin Allergies
Author: Anna Nahirnyak, Pharm.D.
Penicillin is the most commonly documented drug allergy, with around 10% of patients reporting a history of reacting to a penicillin-class antibiotic. However, fewer than 1% of the general population are truly allergic, and most (around 80% of patients) will lose the allergy after 10 years (Joint Task Force on Practice Parameters 2010). This is significant because penicillin allergy mislabeling leads to unnecessary broad-spectrum antibiotic use, increasing the risk of Clostridioides difficile infections, antibiotic resistance, and prolonged hospital stays and higher health care costs (Castells 2019). A 2018 study found that patients labeled as penicillin-allergic had a 50% higher risk of surgical site infections because of the use of second-line perioperative antibiotics (Blumenthal 2018a). Another large cohort study found that a penicillin allergy label was associated with a 69% increased risk of methicillin-resistant Staphylococcus aureus and a 26% increased risk of C difficile infections (Blumenthal 2018b). A 1993 study showed that routine penicillin skin testing enabled the safe administration of penicillin in over 90% of individuals previously labeled as allergic (Gadde 1993). These findings underscore the importance of integrating proactive penicillin allergy de-labeling initiatives into antibiotic stewardship programs to improve patient care (Castells 2019).
Immune reactions to penicillin are mainly antibody mediated (immediate reaction) or T-cell mediated (delayed reaction). As a hapten, penicillin binds to serum proteins in the body, which can trigger allergic reactions. Immediate, IgE-mediated reactions (type I) cause mast cells to release histamine, leading to symptoms such as urticaria, angioedema, bronchospasm, or anaphylaxis. T cell–mediated reactions (type IV) occur hours to weeks after exposure and can cause severe conditions such as drug reaction with eosinophilia and systemic symptoms, Stevens-Johnson syndrome and toxic epidermal necrolysis, or acute generalized exanthematous pustulosis. Of note, many patients may report a penicillin allergy given a family history or previous adverse effects such as headache or isolated GI symptoms; however, these are inconsistent with a true penicillin allergy and should not be documented as such (Castells 2019).
Table 1 summarizes the recommendations on de-labeling penicillin allergies published in the 2022 drug allergy practice parameter update by the American Academy of Allergy, Asthma & Immunology (AAAAI) (Khan 2022). Some patients with a history of nonallergic reactions may be instantly de-labeled by clinicians, whereas others, if deemed at low risk, may bypass penicillin skin testing and proceed directly to a drug challenge. Patients at low risk can be identified using the penicillin allergy clinical decision rule (PEN-FAST) introduced in 2021: 2 points are assigned for an allergic reaction within the past 5 years or for the severe nature of the reaction (eg, anaphylaxis, angioedema, or a severe cutaneous skin reaction), and 1 point is assigned if treatment was required for the allergic reaction or if the treatment history is unknown (Trubiano 2020). Patients with a PEN-FAST score of 2 or less are considered at very low to low risk of a positive penicillin skin test, and they can safely be de-labeled with an oral amoxicillin challenge without preceding skin testing as shown in the 2023 Use of Penicillin Allergy Clinical Decision Rule to Enable Direct Oral Penicillin Challenge (PALACE) trial (Copaescu 2023). Because skin testing and allergy consultations are not universally available and can be costly for patients, pharmacists should feel empowered to de-label patients with a low-risk penicillin allergy. In a study investigating a pharmacist-led, multidisciplinary approach to penicillin allergy de-labeling, 40 of 45 patients at low risk (88.9%) were successfully de-labeled, and 24 (53.3%) were changed to a penicillin antibiotic (Hearsey 2023). The Infectious Diseases Society of America Implementing an Antibiotic Stewardship Program guidelines also emphasize the importance of a multidisciplinary approach and the role of pharmacists in allergy de-labeling (Barlam 2016).
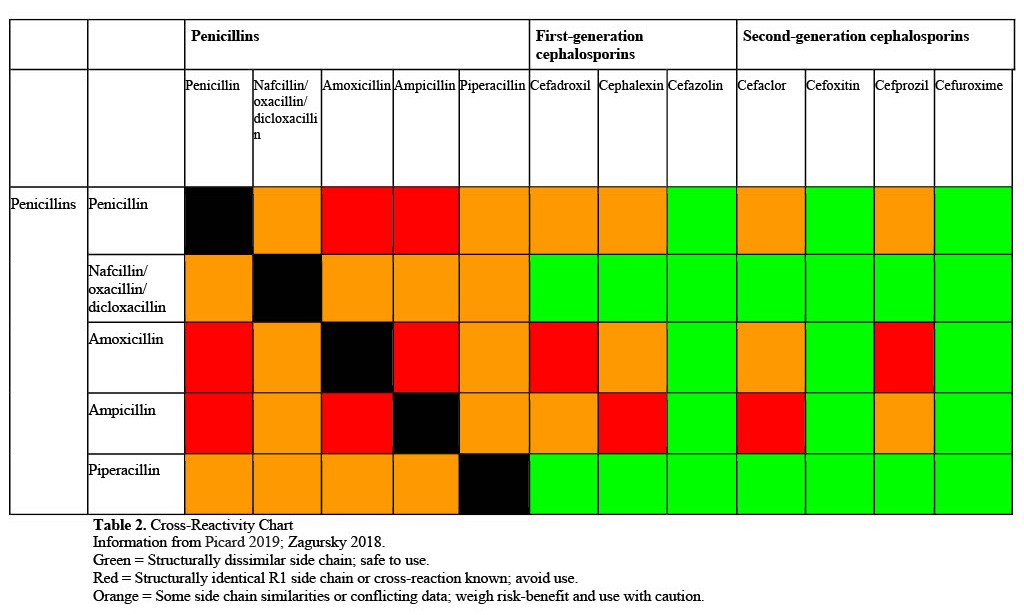
Patients with a true penicillin allergy who require antibiotic therapy may still be able to safely receive an alternative β-lactam antibiotic. Although the β-lactam ring is a common structural feature among penicillins, cephalosporins, carbapenems, and monobactams, differences in their R1 side chain play a key role in determining the extent of cross-reactivity (Castells 2019). According to the most recent findings, the risk of cross-reactivity in patients with a confirmed IgE- or T cell–mediated penicillin allergy was 16.45% for aminocephalosporins with identical side chains, 5.60% for cephalosporins with intermediate similarity, and 2.11% for those with low similarity scores. The risk of cross-reactivity to any carbapenem was very low at 0.87% (Picard 2019). Aztreonam appears to have no immunologic or clinical cross-reactivity with penicillins and most cephalosporins. However, hypersensitivity reactions to aztreonam have been reported in patients allergic to ceftazidime, which shares an identical R1 side chain with aztreonam and cefiderocol. Because of the particularly low risk of cross-reactivity between structurally dissimilar β-lactams, the AAAAI drug allergy practice parameter update recommends that patients with a penicillin hypersensitivity can safely be administered a structurally dissimilar cephalosporin without additional precautions (Khan 2022). Cross-reactivity charts can be used by clinicians to choose a safe alternative cephalosporin in patients with a confirmed penicillin allergy (Table 2) (Picard 2019; Zagursky 2018). An important exception to these recommendations applies to patients who have experienced severe delayed immunologic reactions or organ-specific reactions to β-lactams. Carbapenems can be administered without additional precautions regardless of whether the reaction to a penicillin was anaphylactic. The 2022 AAAAI document includes helpful flowsheets outlining the approach to β-lactam administration or allergy testing in patients with a history of β-lactam allergies according to the type of allergic reaction and the structural similarity of the antibiotics involved (Khan 2022).
In summary, integrating penicillin allergy de-labeling protocols into antimicrobial stewardship is crucial for optimizing antibiotic selection and patient outcomes while minimizing the harms of alternative therapy such as resistance, C difficile infections, and increased costs (Castells 2019; Blumenthal 2018a; Barlam 2016). For patients with confirmed penicillin hypersensitivity without a severe delayed immunologic reaction or organ-specific reaction, use of structurally dissimilar β-lactams ensures effective treatment without compromising patient safety (Khan 2022).
References
Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an antibiotic stewardship program: guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77. https://doi.org/10.1093/cid/ciw118
Blumenthal KG, Ryan EE, Li Y, Lee H, Kuhlen JL, Shenoy ES. The impact of a reported penicillin allergy on surgical site infection risk. Clin Infect Dis. 2018a;66(3):329-336. https://doi.org/10.1093/cid/cix794
Blumenthal KG, Lu N, Zhang Y, Li Y, Walensky RP, Choi HK. Risk of methicillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. BMJ. 2018b;361:k2400. https://doi.org/10.1136/bmj.k2400
Castells M, Khan DA, Phillips EJ. Penicillin allergy. N Engl J Med. 2019;381(24):2338-2351. https://doi.org/10.1056/NEJMra1807761
Copaescu AM, Vogrin S, James F, et al. Efficacy of a clinical decision rule to enable direct oral challenge in patients with low-risk penicillin allergy: the PALACE randomized clinical trial. JAMA Intern Med. 2023;183(9):944-952. https://doi.org/10.1001/jamainternmed.2023.2986
Gadde J, Spence M, Wheeler B, Adkinson NF Jr. Clinical experience with penicillin skin testing in a large inner-city STD clinic. JAMA. 1993;270(20):2456-2463.
Hearsey D, Elkhalifa S, Sandoe J, et al. Removal of incorrect penicillin allergy labels in a UK hospital. Clin Microbiol Infect. 2023;29(10):1338.e1-1338.e4. https://doi.org/10.1016/j.cmi.2023.06.024
Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010;105(4):259-273. https://doi.org/10.1016/j.anai.2010.08.002
Khan DA, Banerji A, Blumenthal KG, et al. Drug allergy: a 2022 practice parameter update. J Allergy Clin Immunol. 2022;150(6):1333-1393. https://doi.org/10.1016/j.jaci.2022.08.028
Picard M, Robitaille G, Karam F, et al. Cross-reactivity to cephalosporins and carbapenems in penicillin-allergic patients: two systematic reviews and meta-analyses. J Allergy Clin Immunol Pract. 2019;7(8):2722-2738.e5. https://doi.org/10.1016/j.jaip.2019.05.038
Trubiano JA, Vogrin S, Chua KYL, et al. Development and validation of a penicillin allergy clinical decision rule. JAMA Intern Med. 2020;180(5):745-752. https://doi.org/10.1001/jamainternmed.2020.0403
Zagursky RJ, Pichichero ME. Cross-reactivity in β-lactam allergy. J Allergy Clin Immunol Pract. 2018;6(1):72-81.e1. https://doi.org/10.1016/j.jaip.2017.08.027
Table 1. Preferred De-labeling Method According to the Nature of the Reported Reaction to Penicillins
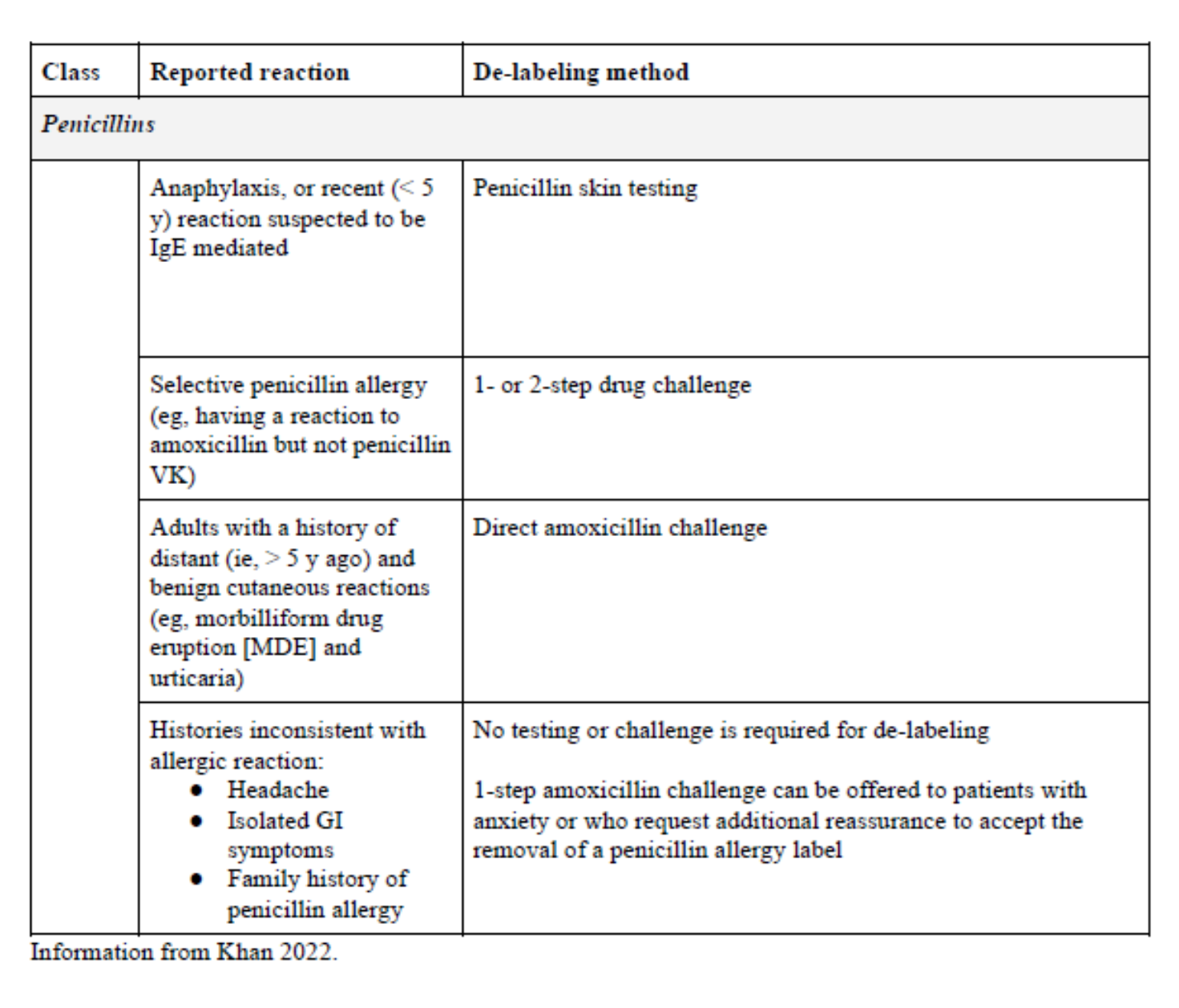 Table 2. Cross-Reactivity Chart
Table 2. Cross-Reactivity Chart
Inspiring the Next Generation of ID Pharmacists Through Digital Innovation
Author: Callan Bleick, Pharm.D., MSc
As the pharmacy profession continues to evolve and the role of infectious diseases (ID) pharmacists expands, the demand for skilled ID specialists is more essential than ever. Innovative digital strategies are pivotal in engaging and inspiring the next generation of pharmacy professionals. The shift from traditional textbooks to modern touchscreens has redefined how learners engage with, absorb, and apply information. With over 90% of millennials owning smartphones and actively navigating multiple digital platforms, educational strategies must adapt to remain relevant and effective (Content Science 2025; Vogels 2023; GWI 2021). Traditionally, didactic lectures with limited clinical exposure have laid the foundation of ID pharmacy education; however, the way students learn is being reshaped through the integration of diverse digital platforms (Bui 2023). Emerging digital tools, such as interactive virtual patient simulation (VPS), artificial intelligence (AI)-driven antimicrobial stewardship and clinical support systems, and popular online media platforms, are revolutionizing learning and advancement in ID pharmacy (Dzintars 2021; Bond 2017).
Virtual Patient Simulation
Interactive VPS, telemedicine platforms, and online learning modules offer real-time learning experiences that enhance clinical decision-making skills and support professional growth. Virtual patient simulations allow students to practice antimicrobial stewardship interventions in a risk-free environment. Justo et al reported that pharmacy students view antimicrobial stewardship as a critical health care priority and express a strong interest in further education on the topic. However, perceptions of antimicrobial coursework and actual knowledge levels differ significantly depending on the pharmacy school attended (Justo 2014). A systematic review found that VPS significantly enhanced higher-level learning, counseling, and decision-making skills more effectively than traditional paper-based cases. In addition, VPS has been shown to improve students’ knowledge and clinical decision-making abilities, particularly in managing complex scenarios (Phanudulkitti 2023; Richardson 2020). These tools can help facilitate an immersive learning experience, reinforcing key concepts in an interactive and engaging way. Because VPS is easily accessible, it can be integrated into pharmacy education regardless of the institution, ensuring students across different programs benefit from this innovative educational approach.
AI and Machine Learning
Artificial intelligence and machine learning are also playing a significant role in shaping the future of ID pharmacy. Artificial intelligence–driven clinical decision support systems (CDSS) help pharmacists analyze vast amounts of patient data to predict antimicrobial resistance patterns and optimize therapeutic regimens (Pinto-De-Sá 2024). A review identified 60 unique machine learning–based CDSS designed to assist ID clinician workflows, with most focused on bacterial infections (62%) and sepsis prediction (30%) (Peiffer-Smadja 2020). However, expanding their inclusion to diverse health care settings is necessary to improve clinical applicability. Artificial intelligence and machine learning can enhance antimicrobial stewardship programs by managing large data sets and automating repetitive tasks, but adoption remains limited because of methodological inconsistencies and a lack of robust, large-scale studies. Furthermore, concerns with overdependence on AI, reduced clinical rationale, and accountability in decision-making present significant challenges to widespread implementation in clinical practice (Mennella 2024; WHO 2023).
Digital Media Platforms
Digital media platforms can enhance formal education while serving as vital tools for professional networking and knowledge exchange. Free-to-use social media channels such as Bluesky, X, LinkedIn, Instagram, TikTok, YouTube, and specialty forums enable learners to collaborate, discuss complex cases, and stay informed on emerging trends in niche health care spaces. Beyond social media, digital platforms also provide educational games, on-demand content, quick reference tools, interactive challenges, and practice tests. Increased engagement during “gameplay” can enhance memory retention, and the adaptable nature of these tools supports group learning and accommodates diverse learning styles (Gauthier 2025a; Pillplexed 2024). In addition, because these platforms are online, content can quickly be updated in response to new guidelines and clinical practices. Game-based learning not only makes studying more enjoyable but has also proved to reduce burnout (JääSkä 2022; Sera 2017). Integrating these tools into pharmacy education enables new learners to develop critical skills and helps bridge the gap between didactic instruction and real-world clinical practice (Gauthier 2025b).
Where Do We Go from Here?
Although digital innovation holds great promise, it is not without challenges. Concerns around misinformation and maintaining evidence-based accuracy remain ongoing issues, especially when learners engage with unregulated, open-access platforms. Infectious diseases pharmacists can help mitigate these risks by sharing credible resources, promoting evidence-based practices, and guiding learners in these digital spaces because involvement reinforces accuracy, fosters critical thinking, and supports clinical integrity. Beyond content oversight, a deeper concern lies in how technology itself is used. Overreliance on technology may hinder the development of critical thinking and clinical reasoning skills. For example, AI-driven tools may streamline decision-making, but they can also introduce new forms of cognitive bias or reduce accountability if not properly supervised. Uneven integration of these technologies across institutions may also exacerbate educational disparities, particularly for students in underresourced settings. In addition, only relying on digital media can interfere with relationship building and the development of communication skills, which are often required for interdisciplinary collaboration and higher-level changes in prescribing. These challenges are further complicated by the lack of generalizability, methodological rigor, and clinical validation. Ultimately, although these innovative tools offer valuable support, they are intended to enhance, not replace, foundational pharmacy education and practice.
Despite these limitations, digital innovation remains a powerful catalyst for progress. When embraced with intention, these tools can enhance education, improve clinical preparedness, and expand access to expert knowledge. As the landscape of health care continues to evolve, so too must our approach to training the next generation. By thoughtfully integrating technological advances, we can ensure ID pharmacists are not only digitally fluent but also clinically adept at navigating the growing complexities of ID. Digital innovation will help guide the next generation of ID pharmacists, and the path forward starts now.
References
Bond SE, Crowther SP, Adhikari S, et al. Design and implementation of a novel web-based e-learning tool for education of health professionals on the antibiotic vancomycin. J Med Internet Res. 2017;19(3):e93. https://doi.org/10.2196/jmir.6971
Bui HP, Ulla MB, Tarrayo VN, Pham CT. Editorial: The roles of social media in education: affective, behavioral, and cognitive dimensions. Front Psychol. 2023;14:1287728. https://doi.org/10.3389/fpsyg.2023.1287728
Content Science. Millennial content consumption fact sheet. 2025. https://review.content-science.com/millennial-content-consumption-fact-sheet/
Dzintars K, Fabre VM, Avdic E, et al. Development of an antimicrobial stewardship module in an electronic health record: options to enhance daily antimicrobial stewardship activities. Am J Health Syst Pharm. 2021;78(21):1968-1976. https://doi.org/10.1093/ajhp/zxab222
Gauthier T. IDstewardship. 2025a. https://www.idstewardship.com/
Gauthier TP, Cady E, Liu T, Landayan AM. Resources and strategies for learning infectious diseases pharmacotherapy during advanced pharmacy practice experiences and pharmacy residency. Am J Health Syst Pharm. 2025b;82(4):228-234. https://doi.org/10.1093/ajhp/zxae250
GWI. Millennials: social media trends report. Consumer Insights Platform; 2021. https://www.gwi.com/reports/millennials-on-social-media
Justo JA, Gauthier TP, Scheetz MH, et al. Knowledge and attitudes of doctor of pharmacy students regarding the appropriate use of antimicrobials. Clin Infect Dis 2014;59 suppl 3(suppl 3):S162-S169. https://doi.org/10.1093/cid/ciu537
JääSkä E, Lehtinen J, Jujala J, Kauppila O. Game-based learning and students’ motivation in project management education. Project Leadership Soc. 2022(3). https://www.mendeley.com/catalogue/8c520d60-314e-3501-9cae-e8bd008a43ef/
Mennella C, Maniscalco U, De Pietro G, Esposito M. Ethical and regulatory challenges of AI technologies in healthcare: a narrative review. Heliyon. 2024;10(4):e26297. https://doi.org/10.1016/j.heliyon.2024.e26297
Peiffer-Smadja N, Rawson TM, Ahmad R, et al. Machine learning for clinical decision support in infectious diseases: a narrative review of current applications. Clin Microbiol Infect. 2020;26(5):584-595. https://doi.org/10.1016/j.cmi.2019.09.009
Phanudulkitti C, Puengrung S, Meepong R, Vanderboll K, Farris KB, Vordenberg SE. A systematic review on the use of virtual patient and computer-based simulation for experiential pharmacy education. Explor Res Clin Soc Pharm. 2023;11:100316. https://doi.org/10.1016/j.rcsop.2023.100316
Pillplexed. About. 2024. https://pillplexed.com/about/
Pinto-De-Sá R, Sousa-Pinto B, Costa-de-Oliveira S. Brave new world of artificial intelligence: its use in antimicrobial stewardship—a systematic review. Antibiotics (Basel). 2024;13(4):307. https://doi.org/10.3390/antibiotics13040307
Richardson CL, White S, Chapman S. Virtual patient technology to educate pharmacists and pharmacy students on patient communication: a systematic review. BMJ Simul Technol Enhanc Learn. 2020;6(6):332-338. https://doi.org/10.1136/bmjstel-2019-000514
Sera L, Wheeler E. Game on: the gamification of the pharmacy classroom. Curr Pharm Teach Learn. 2017;9(1):155-159. https://doi.org/10.1016/j.cptl.2016.08.046
Vogels E, Gelles-Watnick R. Teens and social media: key findings from Pew Research Center surveys. Pew Research Center; 2023. https://www.pewresearch.org/short-reads/2023/04/24/teens-and-social-media-key-findings-from-pew-research-center-surveys/
World Health Organization. WHO outlines considerations for regulation of artificial intelligence for health 2023. https://www.who.int/news/item/19-10-2023-who-outlines-considerations-for-regulation-of-artificial-intelligence-for-health